






 2517 / 2894
2517 / 2894

Tratamiento de rescate sin demora
Las opciones de tratamiento de rescate son intervenciones que
no se han aplicado antes o en las que la vida media sugiere que
ya no son activa
s 190 .Los antagonistas de la serotonina, si no se
administraron en el quirófano, pueden ser el primer tratamiento
en la URPA ya que carecen de efecto sedante. También, aña-
diendo dexametasona al dolasetrón o al haloperidol pueden
aumentar la reducción global de riesgo de precisar tratamiento
de rescate (de nuevo, si no se ha administrado antes
) 193 .Final-
mente, la estimulación del punto P6 de acupresión puede ser una
opción válida, ya que ha demostrado ser eficaz en la prevención
de las NVPO.
Bibliografía
1. Dolin SJ, Cashman JN, Bland JM: Effectiveness of
acute postoperative pain management: I. Evidence
from published data. Br J Anaesth 89:409-423, 2002.
2. Palazzo M, Evans R: Logistic regression analysis of
fixed patient factors for postoperative sickness: A
model for risk assessment. Br J Anaesth 70:135-140,
1993.
3. CohenMM, Duncan PG, DeBoer DP,
TweedWA:Thepostoperative interview: Assessing risk factors for
nausea and vomiting. Anesth Analg 78:7-16, 1994.
4. Koivuranta M, Laara E, Snare L, Alahuhta S: A
survey of postoperative nausea and vomiting.
Anaesthesia 52:443-449, 1997.
5. Apfel CC, Laara E, Koivuranta M, et al: A simplified
risk score for predicting postoperative nausea and
vomiting: Conclusions from cross-validations
between two centers. Anesthesiology 91:693-700,
1999.
6. Eberhart LHJ, Hogel J, Seeling W, et al: Evaluation
of three risk scores to predict postoperative nausea
and vomiting. Acta Anaesthesiol Scand 44:480-488,
2000.
7. Visser K, Hassink EA, Bonsel GJ, et al: Randomized
controlled trial of total intravenous anesthesia with
propofol versus inhalation anesthesia with isoflurane-
nitrous oxide: Postoperative nausea with vomiting and
economic analysis. Anesthesiology 95:616-626, 2001.
8. Stadler M, Bardiau F, Seidel L, et al: Difference in
risk factors for postoperative nausea and vomiting.
Anesthesiology 98:46-52, 2003.
9. Watcha MF, White PF: Postoperative nausea and
vomiting: Its etiology, treatment, and prevention.
Anesthesiology 77:162-184, 1992.
10. Macario A, Weinger M, Carney S, Kim A: Which
clinical anesthesia outcomes are important to
avoid? The perspective of patients. Anesth Analg
89:652-658, 1999.
11. Gan T, Sloan F, Dear G, et al: Howmuch are patients
willing to pay to avoid postoperative nausea and
vomiting? Anesth Analg 92:393-400, 2001.
12. Kerger H, Turan A, Kredel M, et al: Patients’ willing-
ness to pay for anti-emetic treatment. Acta Anaes-
thesiol Scand 51:38-43, 2007.
13. Darkow T, Gora-Harper ML, Goulson DT, Record
KE: Impact of antiemetic selection on postoperative
nausea and vomiting and patient satisfaction. Phar-
macotherapy 21:540-548, 2001.
14. Bremner WG, Kumar CM: Delayed surgical emphy-
sema, pneumomediastinum and bilateral pneumo-
thoraces after postoperative vomiting. Br J Anaesth
71:296-297, 1993.
15. Schumann R, Polaner DM: Massive subcutaneous
emphysema and sudden airway compromise after
postoperative vomiting. Anesth Analg 89:796-797,
1999.
16. Gold BS, Kitz DS, Kecky JH, Neuhaus JM: Unanti-
cipated admission to the hospital following ambu-
latory surgery. JAMA 262:3008-3010, 1989.
17. Hill RP, Lubarsky DA, Phillips-Bute B, et al: Cost-
effectiveness of prophylactic antiemetic therapy
Náuseas y vómitos postoperatorios
2517
76
Sección VI
Cuidados postoperatorios
© ELSEVIER. Fotocopiar sin autorización es un delito
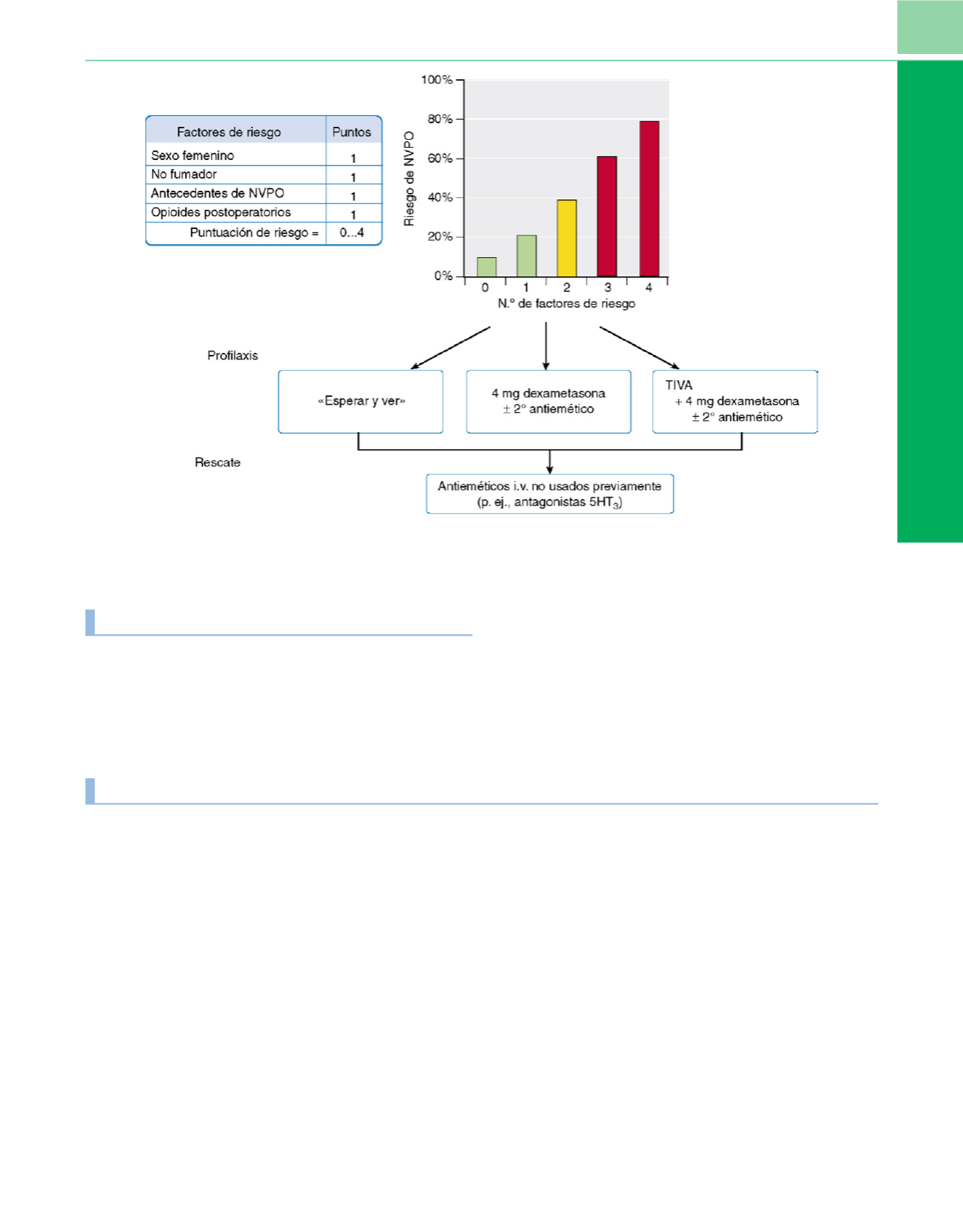
Figura 76-14
Algoritmo para el tratamiento del las NVPO.